
Interesting acute stress disorder facts
Acute stress disorder facts
Acute stress disorder (ASD) is a common and temporary mental disorder people often develop after a traumatic event, such as a traffic accident, a robbery or physical abuse. Feelings of anxiety, fear, powerlessness, and helplessness are common after experiencing a traumatic event. ASD is characterized by reexperiencing the traumatic event and avoiding reminders of the event. If ASD is not managed correctly, it can develop into posttraumatic stress disorder (PTSD). Accurate acute stress disorder facts are difficult to find, because there hasn’t been much research done to this condition compared to other mental disorder (depression or PTSD). However, this page offers a good overview of interesting acute stress disorder facts, all backed up by scientific literature.
Go to:
- What is acute stress disorder?
- What causes ASD?
- Diagnosing ASD.
- ASD treatment.
- How to cope with ASD.
- Helping your partner with ASD.
- Take the ASD test.
- Online counseling for ASD.
- Take me to the homepage.
At Barends Psychology Practice acute stress disorder treatment is offered (also online). Go to contact us to schedule a first, free of charge, first session. (Depending on your health insurance, treatment may be reimbursed).
Acute stress disorder facts – prevalence
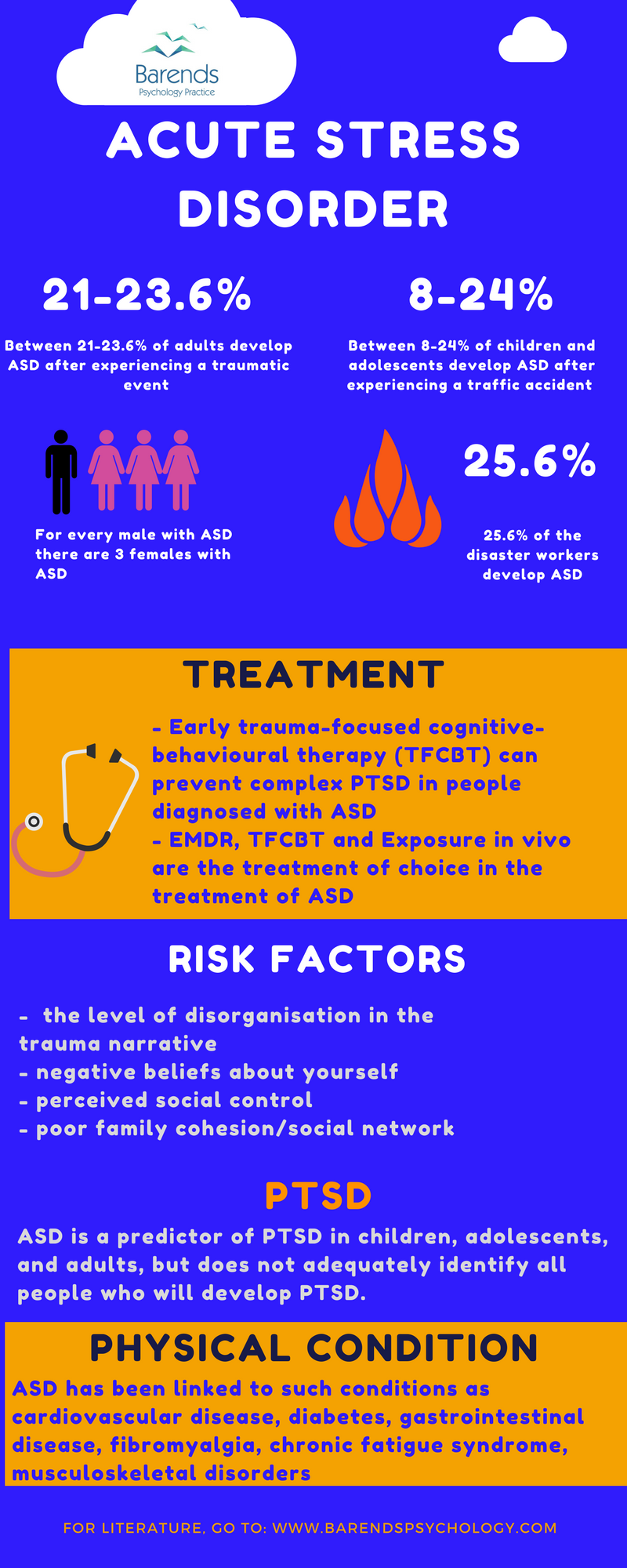
- Between 21% and 23.6% of adults develop ASD after experiencing a traumatic event [11]. Between 8% and 24% (dissociation excluded) of the children and adolescents who were involved in traffic accidents met the criteria for ASD; 14% had subsyndromal ASD [13],[18].
- In another study, 40% of the adolescent trauma survivors met the criteria for ASD, and their quality of life was significantly negatively affected [21].
- ASD was diagnosed more often in women than in men (23% versus 8%). Of these people 57% of men and 92% of women developed PTSD 6 months later [10].
- The nature of potential traumatic events for women (sexual assault and (child) sexual abuse) is more extreme and thus leads more often to the development of ASD and PTSD [3].
- Men are more likely than women to report experiencing accidents, non sexual assault, war or combat,
serious illness or unspecified injury, disaster or fire, and witnessing death or injury [3].
Acute stress disorder facts – exposed disaster workers
- Exposed disaster workers (of 09/11) had higher rates of acute stress disorder (ASD) compared to the normal population (25.6% versus 2.4%) [1]
- Younger exposed disaster workers were more likely to develop ASD compared to older exposed disaster workers [1].
- Unmarried exposed disaster workers were 2.26 times more likely to develop ASD compared to married exposed disaster workers [1].
- Exposed disaster workers with ASD were 7.33 times more likely to develop PTSD comared to those without ASD [1].
Acute stress disorder facts – symptoms and risk factors
- More than half of the people with ASD experience panic symptoms and score higher on the anxiety sensitivity index than people without ASD [4]. This suggests that peritraumatic panic could be related to PTSD.
- In children, there are two predictors for acute stress disorder: the level of disorganisation in the trauma narrative, and the child’s cognitive appraisals of the event [5]. Children with ASD are more disorganized in their narrative of the traumatic event.
- 3 aspects of trauma narrative disorganization (repetition, non-consecutive chunks, and coherence) are also predictors of ASD and PTSD in adults [7] and won’t necessarily disappear when ASD disappears [7].
- People with ASD displayed more negatieve beliefs (about their functioning) after the trauma, and reported higher levels of anxiety symptoms than people not diagnosed with ASD [8]. In other words, people who have a lot of negatieve beliefs about themselves, are more likely to develop ASD or PTSD.
- Peritraumatic dissociation and ASD is a more accurate predictor of PTSD in females than males [10]. The reasons behind this gender difference is still unclear.
- Perceived social control and negative social support are good predictors of ASD and PTSD [11]. This is in line with another study [12] where family cohesion and expressiveness are related with less psychological distress and ASD [12].
- ASD and PTSD have been linked to such conditions as cardiovascular disease, diabetes, gastrointestinal disease, fibromyalgia, chronic fatigue syndrome, musculoskeletal disorders, and other diseases. Evidence linking cardiovascular disease and exposure to psychological trauma is particularly strong and has been found consistently across different populations and stressor events.[2]
- ASD is a predictor of PTSD in children and adolescents [13] and in adults [14],[15]. However, greater emphasis on reexperiencing, avoidance, and arousal symptoms will increase the predictive power [14].
- According to a systematic review of 2011, ASD is a predictor of PTSD, but it does not adequately identify the people who will develop PTSD [16]. Greater emphasis should be placed on describing the broad range of initial reactions. Taking the above mentioned bullet points into consideration, it seems clear that the diagnosis of ASD alone is not strong enough of a predictor of PTSD.
- Adolescent trauma survivors’ quality of life improves significantly if they received treatment for their ASD soon after the traumatic event [21].
- Both CBT and CBT-hypnosis significantly reduce posttraumatic stress symptoms. CBT-hypnosis resulted in greater reduction of reexperiencing symptoms than CBT [6].
- Early trauma-focused cognitive-behavioural therapy (TFCBT) can prevent complex PTSD in people diagnosed with ASD [9], and is successful in treating ASD [9],[17]. This finding suggests that it could be benefical to offer TFCBT to people diagnosed with ASD.
- Exposure in vivo significantly reduce ASD symptoms. At the end of treatment, only 12% had the diagnosis of PTSD [17].
- EMDR, TFCBT and Exposure in vivo are the treatment of choice in the treatment of ASD and PTSD [17],[18].
(Advertisement. For more information about ASD, please scroll down).
Acute stress disorder – ASD in relation to PTSD
Acute stress disorder facts – treatment
(Advertisement. For more information about ASD, please scroll down).
Literature
- [1] Fullerton, C. S., Ursano, R. J., & Wang, L. (2004). Acute stress disorder, posttraumatic stress disorder, and depression in disaster or rescue workers. American Journal of Psychiatry, 161, 1370-1376.
- [2] Boscarino, J. A. (2004). Posttraumatic stress disorder and physical illness: results from clinical and epidemiologic studies. Annals of the New York Academy of Sciences, 1032, 141-153.
- [3] Tolin, D. F., & Foa, E. B. (2006). Sex differences in trauma and posttraumatic stress disorder: a quantitative review of 25 years of research. Psychological bulletin, 132, 959.
- [4] Bryant, R. A., & Panasetis, P. (2001). Panic symptoms during trauma and acute stress disorder. Behaviour Research and Therapy, 39, 961-966.
- [5] Salmond, C. H., Meiser‐Stedman, R., Glucksman, E., Thompson, P., Dalgleish, T., & Smith, P. (2011). The nature of trauma memories in acute stress disorder in children and adolescents. Journal of Child
Psychology and Psychiatry, 52, 560-570. - [6] Bryant, R. A., Moulds, M. L., Guthrie, R. M., & Nixon, R. D. (2005). The additive benefit of hypnosis and cognitive-behavioral therapy in treating acute stress disorder. Journal of Consulting and Clinical Psychology, 73, 334.
- [7] Jones, C., Harvey, A. G., & Brewin, C. R. (2007). The organisation and content of trauma memories in survivors of road traffic accidents. Behaviour research and therapy, 45, 151-162.
- [8] Nixon, R. D., & Bryant, R. A. (2005). Are negative cognitions associated with severe acute trauma responses? Behaviour Change, 22, 22-28.
- [9] Kornør, H., Winje, D., Ekeberg, Ø., Weisæth, L., Kirkehei, I., Johansen, K., & Steiro, A. (2008). Early trauma-focused cognitive-behavioural therapy to prevent chronic post-traumatic stress disorder and related symptoms: a systematic review and meta-analysis. BMC psychiatry, 8, 81.
- [10] Bryant, R. A., & Harvey, A. G. (2003). Gender differences in the relationship between acute stress disorder and posttraumatic stress disorder following motor vehicle accidents. Australian & New Zealand Journal of Psychiatry, 37, 226-229.
- [11] Holeva, V., Tarrier, N., & Wells, A. (2001). Prevalence and predictors of acute stress disorder and PTSD following road traffic accidents: Thought control strategies and social support. Behavior Therapy, 32, 65-83.
- [12] Shaw, R. J., Deblois, T., Ikuta, L., Ginzburg, K., Fleisher, B., & Koopman, C. (2006). Acute stress disorder among parents of infants in the neonatal intensive care nursery. Psychosomatics, 47, 206-212.
- [13] Meiser-Stedman, R., Yule, W., Smith, P., Glucksman, E., & Dalgleish, T. (2005). Acute stress disorder and posttraumatic stress disorder in children and adolescents involved in assaults or motor vehicle accidents. American Journal of Psychiatry, 162, 1381-1383.
- [14] Harvey, A. G., & Bryant, R. A. (2000). Two-year prospective evaluation of the relationship between acute stress disorder and posttraumatic stress disorder following mild traumatic brain injury. American Journal of Psychiatry, 157, 626-628.
- [15] Classen, C., Koopman, C., Hales, R., & Spiegel, D. (1998). Acute stress disorder as a predictor of posttraumatic stress symptoms. American Journal of Psychiatry, 155, 620-624.
- [16] Bryant, R. A. (2011). Acute stress disorder as a predictor of posttraumatic stress disorder: a systematic review. The Journal of clinical psychiatry.
- [17] Ponniah, K., & Hollon, S. D. (2009). Empirically supported psychological treatments for adult acute stress disorder and posttraumatic stress disorder: a review. Depression and anxiety, 26, 1086-1109.
- [18] Forbes, D., Creamer, M., Phelps, A., Bryant, R., McFarlane, A., Devilly, G. J., … & Newton, S. (2007). Australian guidelines for the treatment of adults with acute stress disorder and post-traumatic stress disorder. Australian & New Zealand Journal of Psychiatry, 41, 637-648.
- [19] Kassam-Adams, N., & Winston, F. K. (2004). Predicting child PTSD: The relationship between acute stress disorder and PTSD in injured children. Journal of the American Academy of Child & Adolescent Psychiatry, 43, 403-411.
- [20] McKibben, J. B., Bresnick, M. G., Wiechman Askay, S. A., & Fauerbach, J. A. (2008). Acute stress disorder and posttraumatic stress disorder: a prospective study of prevalence, course, and predictors in a sample with major burn injuries. Journal of burn care & research, 29, 22-35.
- [21] Holbrook, T. L., Hoyt, D. B., Coimbra, R., Potenza, B., Sise, M., & Anderson, J. P. (2005). High rates of acute stress disorder impact quality-of-life outcomes in injured adolescents: mechanism and gender predict acute stress disorder risk. Journal of Trauma and Acute Care Surgery, 59, 1126-1130.